


At the Brown University Pandemic Center, doctors are following the current Ebola outbreak in central Africa with expertise as well as empathy.
“Initial case counts were incredibly high… with case counts at declaration larger than most outbreaks when they end,” said Dr. Craig Spencer, an emergency medicine physician who survived a case of Ebola in 2014 during an outbreak that caused 11,308 deaths. “There has been some noticeable improvement in testing and other capacities, but it still feels like the early days, in which there’s a lot of uncertainty.”
With over 500 confirmed cases and counting, Brown University experts said this “will likely be the second largest Ebola outbreak ever recorded.” Medical response is improving in the area to contain and track the disease, but there are no approved vaccines or treatments for this particular strain of Ebola, the Bundibugyo virus (BDV). The Pandemic Center said Ebola is very unlikely to reach Providence via the World Cup because of travel restrictions, the method of transmission and the remote location of the outbreak.
Providence Welcomes International Tourists, with Ebola Transmission Risks Low
On May 17, the World Health Organization declared an international health emergency for BDV. They reported over 200 confirmed cases of the virus in the Democratic Republic of the Congo and a handful in Uganda. At the time, Africa Centres for Disease Control and Prevention director general Jean Kaseya estimated there could be more than 1,000 cases.
The next day, May 18, the U.S. temporarily blocked certain non-U.S. citizens who traveled in the DRC, South Sudan or Uganda within the last 21 days. This includes green card holders, who have historically been exempt from similar orders and travel bans. Although Providence expects thousands of international travelers to arrive for World Cup matches, Spencer said Ebola should not be a major concern for people in Providence.
“I think those restrictions do make it less likely, of course, that there’s going to be importation, but the bigger reality is that the last thing that you’re gonna do, if you have Ebola, is want to get on a plane,” said Spencer. “But for me, Ebola is not the number one or number two or even number three threat for me as we are seeing an importation of a lot of folks coming here primarily for the World Cup.”
As of June 8, the DRC confirmed there have been 515 Ebola cases with 91 related deaths. On June 6, Uganda reported 19 cases, including two deaths. The Brown Pandemic Center called for increased capacity for local medical teams, who need personal protective equipment and the training to use them properly. However, these outbreaks are located in places that are difficult to travel to, and unlike respiratory viruses such as COVID and the flu, Ebola is only transmitted through body fluids and contaminated objects.
“One fortunate thing about this virus is you’re most contagious when you’re really quite ill,” said Dr. Jennifer Nuzzo, director of the Pandemic Center at Brown’s School of Public Health. “So it’s not like COVID, where you could be sitting next to someone who doesn’t even know they’re infected and perhaps contract the virus.”
The Rhode Island Department of Health said authorities are regularly communicating with healthcare partners about monitoring travel-associated infections. Officials also said they are keeping an eye on specific disease risks dependent on visitors’ countries of origin.
“Through the Rhode Island State Health Laboratories, syndromic surveillance (monitoring things like symptoms, emergency department visits, wastewater to predict outbreaks before we have a confirmation from lab testing), a rotation of on-call physicians, epidemiologists, and nurses, and RIDOH’s emergency preparedness team, RIDOH monitors reportable infectious diseases, locates people who have been exposed, and guides them to preventive and protective action,” said Public Information Officer Joseph Wendelken.
Nuzzo expressed concerns that a new U.S. plan to quarantine Americans in Kenya will “drive exposures underground,”and that imposing severe travel restrictions could make it less likely relevant information is reported and more difficult for U.S. to send healthcare workers to contain the risk. While the U.S. has dedicated over $162 million dollars in foreign assistance to combat the current outbreak, the largest donor, former U.S. officials and on the ground healthcare workers said funding cuts to the World Health Organization and foreign aid to the DRC negatively affected Ebola detection and containment.
“So I don’t know how we’re gonna end this outbreak, not only if the U.S. doesn’t show up financially and logistically, but if other countries don’t as well,” said Nuzzo, who also said she could not point to who was in charge of the U.S. Ebola response. “I think that’s a function of someone not having been explicitly named, but also because of really stunning vacancies throughout our federal health agencies, at every level. We don’t have a CDC director in place. Many of the senior level positions at FDA [and] HHS are vacant.”
What About Hantavirus, COVID-19 or Measles?
Spencer points out that even when high consequence pathogens like Ebola enter the United States, there are 13 hospitals all around the country that can handle those types of diseases—including Massachusetts General Hospital in Boston. Still, there are other diseases to be watching out for this summer.
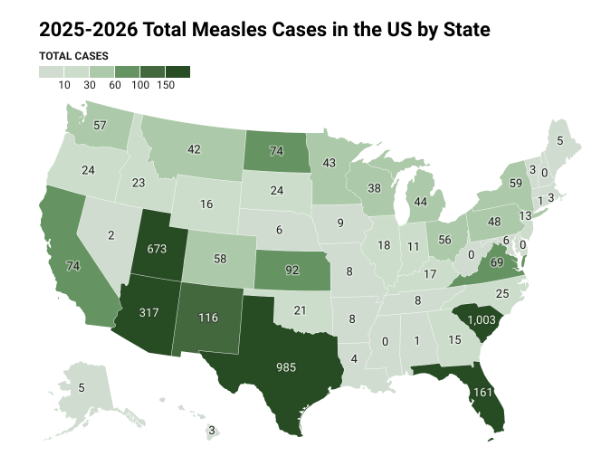
“I am concerned about the importation of measles,” said Spencer. “I am much more concerned about importation of other infectious threats. They may not seem as scary to us as Ebola.”
Since the beginning of 2026, 2,218 measles cases have been recorded in the United States, already passing the number of cases recorded over the entire year of 2025. In November, the Pan American Health Organization will decide whether to revoke the United States status of eliminating the disease.
Over the past year, only 3 measles cases were reported in Rhode Island. The state has a degree of “herd immunity” because 97% of kindergarteners have received vaccines for measles, mumps, and rubella (MMR).
Wendelken dismissed concerns of hantavirus, an infection transmitted through contact with urine, feces, or saliva of infected rodents and contaminated surfaces. The disease made international headlines after an outbreak on the MV Hondius cruise ship caused three deaths. Wendelken said Rhode Islanders are at “very low risk.”
“Hantavirus is extremely rare in Rhode Island. There are many different kinds of hantavirus and of these, only one (the Andes virus strain) can spread from person to person,” said Wendelken. “There has never been a case of Andes virus in Rhode Island, and even with the Andes virus, person-to-person transmission is uncommon and limited to people with close, prolonged contact with an infected person.”
Meanwhile, COVID-19 activity is at the lowest levels recorded in the past 12 months. However, if trends mimic what occurred in 2025, there could be an increase in COVID-19 cases that begin to rise in mid-June that peaks by late August and early September.
Seasonal influenza, or flu, is also currently decreasing. This winter, the CDC reported the third-highest hospitalizations for flu since 2010-2011. In the week ending on May 30, 2026, five children in the U.S. died from the flu—increasing the 2025-2026 child death toll from the disease to 179 deaths. Of those children, the Pandemic Center reports 85% of them were not fully vaccinated against the flu.
To stay up to date on disease risk in the United States, subscribe to the Brown Pandemic Center’s weekly tracking reports of major diseases.
Eric Halvarson is the City News Reporter for The Providence Eye.
Want to comment? Click!