



With the collapse of Anchor Medical in mid-2025, leaving over 25,000 patients scrambling to find new primary care providers, Rhode Island’s ability to attract and keep healthcare entities afloat in New England’s competitive healthcare market has come into question. Many believe subpar reimbursement rates are the reason for the Ocean State’s lack of providers.
Broadly defined, reimbursements are the payments made by insurance companies to medical providers for services like annual checkups or urgent care visits. These rates of reimbursements are either negotiated between healthcare providers and private insurers or, for Medicaid and Medicare, set by the state and federal government, respectively.
Just like in any market, the going price for healthcare services attracts healthcare entities to meet the demand for them. As businesses like Anchor Medical have floundered, many have asked: If Rhode Island’s public sector insurance (Medicaid and Medicare) and private insurers are not able to reimburse at rates commensurate with those in nearby states, how will RI attract healthcare entities and individual providers to keep pace with demand?
Neronha Sounds the Bell Over Reimbursement Rates
Rhode Island Attorney General Peter Neronha, in a live panel discussion with the Boston Globe, described Rhode Island’s reimbursement structure as a “fundamental problem,” in the state’s healthcare economy, raising alarm bells about low reimbursement rates failing to support primary care in Rhode Island.
He continued, “There’s just not enough revenue coming into the system…if we don’t bring up our Medicaid rates, if we don’t bring up our Medicare rates, if we don’t bring up commercial [rates] too…our system is going to have spectacular failure.”
In the same discussion, Neronha highlighted the need to increase Medicaid funding especially, stating that for the same primary care check-up visit, a provider would receive $200 from a private insurer, $100 from Medicare (usually reserved for those who are over 65 years old, permanently disabled, or both) and $37 from Medicaid. With 21% and 17% of Rhode Islanders on Medicaid and Medicare respectively—both numbers are a percentage point or two higher than their corresponding national averages—it’s no wonder that these low reimbursement rates constitute a major challenge for the success of the healthcare industry.
The hypothesis here is that low reimbursement rates translate to lower pay for physicians and other clinicians, making it harder for RI to attract and retain healthcare employees.
Is Competition from Neighboring States Really the Problem?
But simply pointing the finger at low reimbursement rates from Medicaid and Medicare is insufficient to explain our supposed inability to compete with our New England neighbors—after all, public insurance reimburses less than private across the board, regardless of geography. In examining the assertion that competition with neighboring states’ reimbursement rates is driving healthcare providers out of Rhode Island, it’s worth asking two questions:
First, does our population disproportionately utilize lower-paying public insurance? Medicare enrollment is 16% in both Connecticut and Massachusetts, virtually the same as in Rhode Island. Medicaid enrollment in Massachusetts is approximately the same as Rhode Island’s, while Connecticut’s is slightly lower at 15%. Given these statistics, the answer is no, RI does not disproportionately rely on public insurance compared to neighboring states.
The second question then is: Regardless of usage rate, are RI’s public and private reimbursement rates for primary care lower in general than other states? In short, the answer is “Yes” for private insurance, and “Maybe” for public ones.
In a 2024 analysis of 2020 claims data conducted by the Rhode Island Foundation, the average private insurance reimbursement in Rhode Island for a standard outpatient visit was $188, compared to $202 in Massachusetts and $266 in Connecticut. On the public insurance side, Medicare payments structures are largely similar across states for Medicare Parts A and B, while Medicaid reimbursements and reimbursement for Medicare Parts C and D (Medicare Advantage and drug costs) can vary considerably.
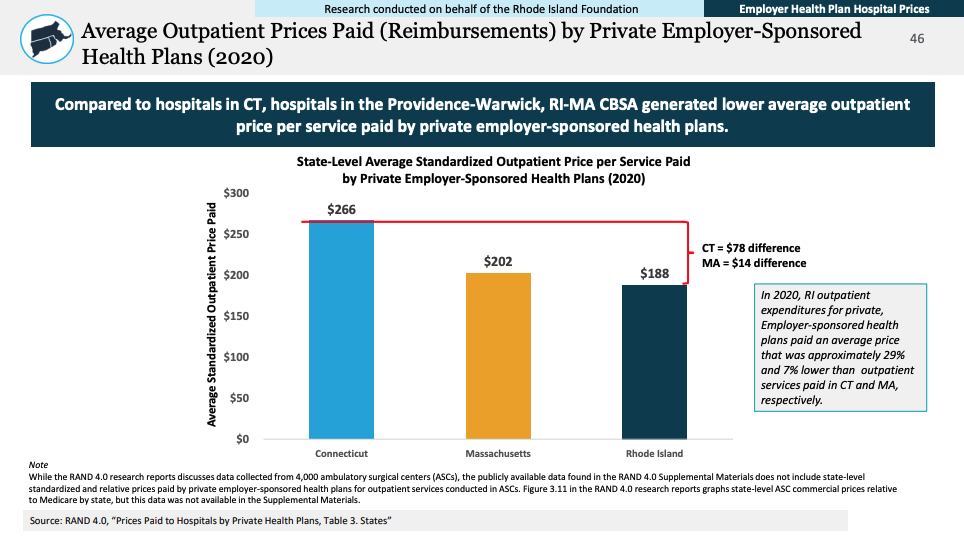
In summary, it appears that our private insurance reimbursement rates are lower than our neighbors, but Rhode Island public insurance rates don’t appear to be much worse.
RI Health Commissioner’s Perspective — Is the Grass Really Greener in Neighboring States?
The focus on state-to-state reimbursement rate discrepancies might be overblown, according to Rhode Island Health Commissioner Cory King.
In an interview with The Providence Eye in July of 2025, Commissioner King stressed that while pricing variability does exist, the disparities in reimbursement rates are driven largely by cost-of-living outliers in the Metro Boston area, saying “Massachusetts has two fee schedules for Medicare. There’s one for Metro Boston—those rates are about 7% higher [for] Medicare—the rest of Massachusetts though, those payments are only about half a percent higher. Connecticut is about 3% higher.”
Overall, Commissioner King stresses that, just as regional economies vary, so will prices—therefore, a lower reimbursement rate does not necessarily spell doom for a healthcare market where the cost of living is also lower. Moreover, Rhode Island offers lower healthcare premiums that correspond with lower reimbursement rates, to the benefit of employers and purchasers of Medicare Advantage plans.
Where Does This Leave RI Patients?
Returning to Anchor Medical’s failure and Attorney General Neronha’s warning that it may prove to be a harbinger of collapse in Rhode Island’s primary care sector: It’s hard to refute the claim that low revenue is a challenge in primary care and medicine as a whole.
However, the statistics don’t seem to bear out the claim that it’s our state that suffers disproportionately when compared to others in New England. While the data shows that our reimbursement rates for primary care may lag in some areas, recent Rhode Island legislation has been proactive in addressing these shortcomings.
Rhode Island’s 2026 budget included $40 million in state and federal funding to support Medicare rate increases for primary care providers. In addition, the budget authorized its Office of the Health Insurance Commissioner (OHIC) to conduct a rate review of its Medicaid plans, potentially opening the door for further increasing rates.
For now, it’s worth widening our view beyond Lil Rhody’s nearby borders to understand that, far from being alone in our struggle to sustain primary care providers, we are among a national effort to do so.
“Last month I was in Connecticut one day and I was in Massachusetts another day and people in both states are talking about how bad access to primary care [is],” said Commissioner King at the end of our interview.
“Sometimes I wonder if we get a little myopic in Rhode Island. The question maybe is, well, is the entire country having a primary care crisis and we just experience it in Rhode Island?”
Charlie Keys McKay is a Providence transplant by way of California and a rising 4th year medical student in Warren Alpert Medical School’s Primary Care-Population Medicine program. Outside of his studies, he enjoys exploring Rhode Island’s food scene, walking and riding the East Bay Bike Path, and reading.
Want to comment? Click!